
Type of publication:
Poster presentation
Author(s):
*Zuydam AC, Rogers SN, Grayson, *McLaughlin K, *Probert, Voyce C
Citation:
British Association of Health and Neck Oncologists, BAHNO Annual Scientific Meeting, Royal College of Physicians, London, Friday 12th May 2017
Abstract:
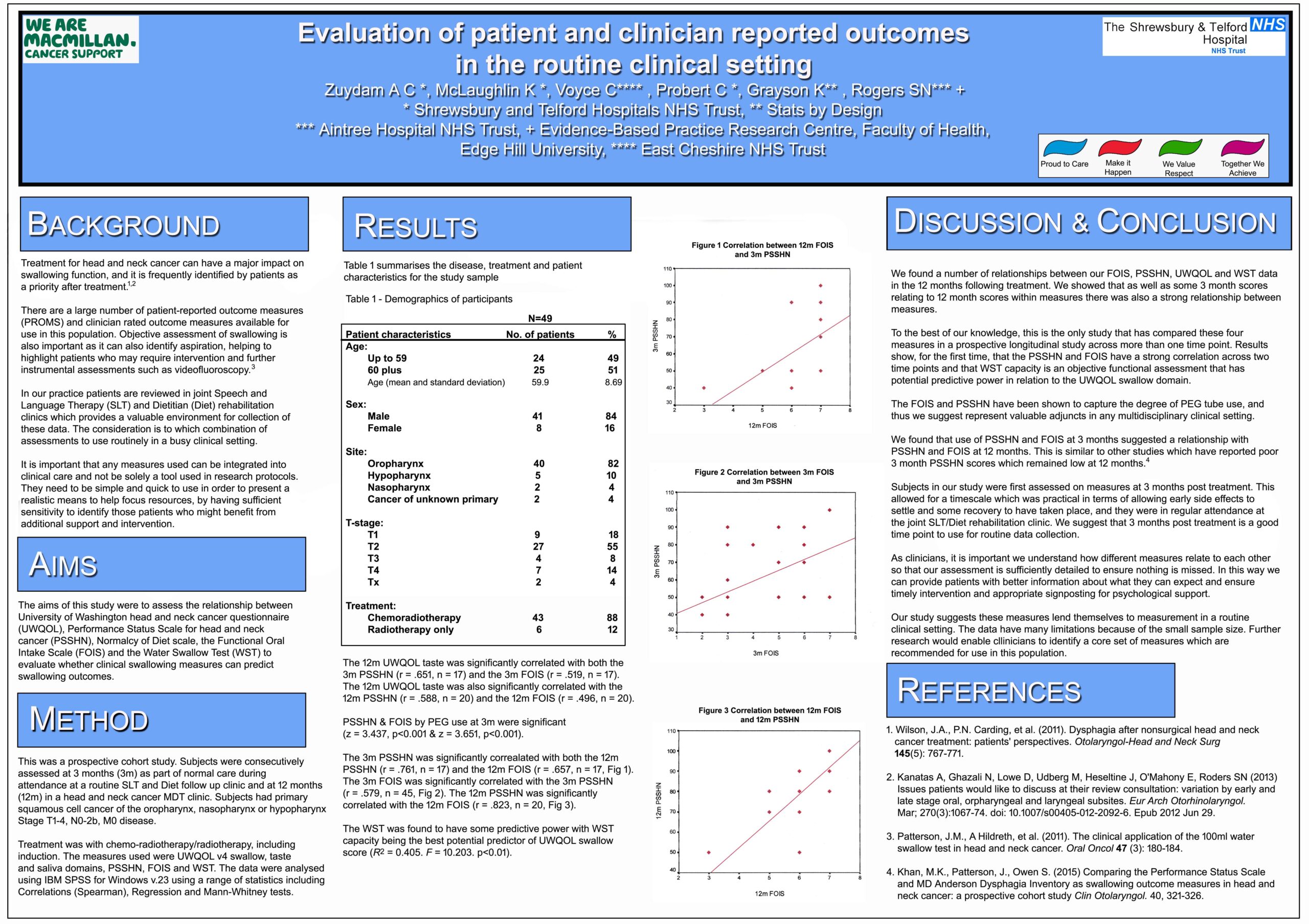
Treatment for head and neck cancer can have an impact on both swallowing function ,and quality of life. It is important that any measures used have sufficient sensitivity to highlight issues .The aims of this study were to assess the relationship between swallowing assessments and to evaluate whether clinical swallowing measures can predict swallowing outcomes.
Methods
This was a prospective cohort study. Subjects had Primary Squamous cell cancer of the oropharynx, nasopharynx or hypopharynx Stage T1‐4, N0‐ 2b, M0 disease. Treatment was with Chemo‐radiotherapy/ radiotherapy ,including induction.The measures used were University of Washington Quality of Life Questionnaire , Performance Status Scale Head and Neck Cancer ( PSSHN) Functional Oral Intake Scale( FOIS ) and the Water Swallow Test ( WST).
Results
Data were collected on 38 patients. The 3m PSSHN was significantly correlated with both the 12m PSSHN (r = .761) and the 12m FOIS (r = .657 ).The 3m FOIS was correlated with the 3m PSSHN (r = .662 ).The 12m PSSHN was significantly correlated with the 12m FOIS (r = .823). The WST was also found to potentially have some predictive power.
Conclusions
A number of measures were found to have clinical significance, and could be valuable to collect in a clinic setting.. Identification of relevant issues early on can enable clinicians to provide patients with information about what they can expect ,and ensure intervention is timely.
Link to poster [no password required]

{kind=link}